What will I do to rehabilitate from a concussion?
Returning to sport, work or everyday activities after a concussion requires a specific return to activity plan that is closely monitored for the re-appearance of concussion signs and/or symptoms. Your Physical Therapist at STAR Physical Therapy, along with consultation from your treating doctor, can create, implement, and monitor your return to activity plan. If you are a student, it is recommended that your health care professional contact your school to ensure they are aware of the recent concussion and to also ensure they are on-board with Return to Learn and Return to Activity guidelines. It is pertinent that all involved in the care of a concussed patient follow the same conservative guidelines in order to optimize recovery.
The backbone of rehabilitating from a concussion is rest until symptoms subside, then a graduated return to cognitive and physical activity without creating any symptoms.
Returning to work or sport following a concussion proceeds through a basic sequential process. Your Physical Therapist will specifically guide you regarding the amount of activity you should engage in and will closely monitor you for signs or symptoms to ensure the healing brain is ready for each progressive level of physical or cognitive activity.
As a general guideline, the steps in this sequential process are:
- No activity, complete cognitive and physical rest
- Light aerobic activity; exercise such as walking or stationary cycling and/or light cognitive activity such as reading or computer work for a short period
- Sport-specific training such as running and/or work/school specific tasks such as working on spreadsheets, solving math problems, or engaging in more mentally challenging tasks
- Non-contact training drills for athletes, more intensive or longer duration physical activity for non-athletes (longer walks) and mental activities of longer duration or combined mental activities such as reading with the television on
- Once cleared by a doctor, athletes begin with full-contact training. Non-athletes are medically cleared to begin back to some regular everyday activity
- Return to competition for athletes at a graduated level (ie: athlete returns to play in one quarter or only on certain offensive/defensive plays.) Non-athletes return to work/school gradually (ie: half days to start or fewer cognitive tasks during a full day).
Each of the 6 stages of the general return to activity plan will occur over a 24-hour period, which means that for athletes suffering a concussion, full return to sport will not occur earlier than approximately 6-7 days after the initial injury. If at any stage during rehabilitation signs or symptoms arise, your Physical Therapist will ask you to cease the current activity and return to resting for a minimum of 24-hours, or until all symptoms have resolved. Activity will begin again once all symptoms have subsided.
Cognitive and physical tasks should begin again at the same level where no symptoms occurred (it is not necessary to return all the way back to stage one unless it is the progression to step two that has caused the symptoms) and proceed then to the next level only once the task at hand has been completed without generating signs or symptoms. Each step can be progressed if it is undertaken without any symptoms arising during or after the exertion, and your Physical Therapist is content with all aspects of your exertion ability and your physical response to this exertion. It is worth mentioning again that no step should be progressed earlier than 24-hours after the previous step. Latent signs and symptoms may appear within this time frame so it is important to allow sufficient time for these to emerge, but also to give the brain time to recover from the exertion it has endured during the rehabilitation process itself.
By following a progressive sequence of increased physical and mental exertion you will be allowed (and encouraged) to exert yourself during rehabilitation as long as this exertion does not bring on signs or symptoms. In other words, exertion both physically and mentally during rehabilitation should be sub-maximal and below a symptom threshold. As mentioned above, in some cases a longer rehabilitation with a longer return to activity plan may be necessary; such as when loss of consciousness was greater than one minute, or in patients who have had repetitive concussions. In these cases, patients may find that they must continue doing activity at one threshold for longer than the 24-hour period while the brain heals. Allowing an athlete to exercise sub-maximally while recovering from a concussion (rather than not exercising at all) is very beneficial to maintain their fitness and psychological state while sitting out with an injury.
While engaging in your rehabilitation plan, it is important to remember that any additional physical or cognitive activity outside of this plan adds to the stress that the healing brain must endure. Going to the movies, completing your taxes, or walking around the shopping centre for the day will all add stress to your healing brain. It is best to report all extracurricular activity that you anticipate engaging in, or need to engage in, to your Physical Therapist so they can take this into account when developing and modifying your rehabilitation plan.
Your Physical Therapist at STAR Physical Therapy will be fundamental in guiding your rehabilitation and return to activity plan after a concussion. They will provide you with criteria regarding the levels of physical and mental exercise to work towards, and will also monitor physical exertion signs, such as your heart and breathing rate, in order to appropriately progress your physical exertion levels from light through to heavy. Your symptoms will be documented in order to monitor for any changes with increasing levels of exertion. Special tests for balance and physical coordination may be used to give your therapist an indication of your physical ability as you recover. Your Physical Therapist will also analyze your individual circumstances and specifically tailor your return to activity to incorporate any special circumstances that may apply to you. For instance, if you are returning to a sport, such as soccer, where the risk of a second concussion is high, your Physical Therapist may delay your return to play for a longer period than if you are returning to a sport such as tennis, or not returning to any sport, but rather a work or scholastic situation where your risk for a second concussion is low or none at all. Factors such as your gender, your predisposition to migraines, learning disabilities, and any previous concussions sustained will also be taken into consideration when tailoring your individual rehabilitation plan.
If you received any concurrent injuries when you sustained your concussion, such as a soft tissue injury to your neck or any other injury, your Physical Therapist at STAR Physical Therapy will simultaneously treat this injury. Your therapist will ensure that not only your brain is ready and prepared to return to your regular activity, but that the rest of your body is also ready to begin. Manual therapy, massage, electrical modalities and specific exercises may be used to treat your neck. It should be noted that in some cases hands-on treatment to the neck area after a concussion can bring symptoms on. Your therapist will closely monitor for this, and treatment will be modified accordingly.
Each patient is unique in both their concussion signs and symptoms, as well as in the sport or job they need to return to, therefore close and frequent monitoring of your return to activity plan by your Physical Therapist is necessary. Your Physical Therapist at STAR Physical Therapy will be in close consultation with your doctor and any other health care professionals that have been involved in the care of your concussion injury to ensure you are returning to your regular activity as quickly but also as safely as possible. Medical clearance from your doctor will be needed before certain levels of activity are undertaken. For those returning to sport, your therapist may also consult with your coach to discuss implementing a gradual return to activity within your practices and matches.
It is worth mentioning again that full recovery from a concussion involves the ability to both physically as well as cognitively handle complex tasks without creating any symptoms. Decreased cognitive function is more easily overlooked than physical symptoms and therefore special attention will be paid by your Physical Therapist to your cognitive function as you recover. Your therapist may use neurocognitive testing to get an objective measure of where your reaction time is at, or to ensure that mentally challenging tasks do not provoke symptoms.
Variables such as stress in a job or the stress of an important sporting event can add to the cognitive demands of any task at hand so these variables will be taken into consideration by your Physical Therapist when your return to activity plan is being implemented. Other variables such as noise and lights can easily aggravate symptoms so will also be taken into account when in the final stages of returning to full activity. For instance, the music and lights during a dance/stage performance, the bright lights of a nighttime playoff game, a match within a large busy stadium, or an office/classroom that is lit with fluorescent lighting can aggravate symptoms. Where possible, your Physical Therapist will attempt to incorporate your regular sporting or work environment into your return to activity plan to ensure the activities you engage in are as similar as possible to those you will incur in your normal environment once you are fully back into action.
If even mild signs or symptoms resulting from the concussion are lingering it is absolutely critical that you do not return to regular activity or sport, particularly where the possibility of incurring another concussion is present. If you do return to activity, the risk of sustaining a second and more damaging concussion is increased as your lagging cognitive function and reduced reaction time leaves you more vulnerable to a second injury. This is termed Second Impact Syndrome.
Second Impact Syndrome
Second-impact syndrome (SIS) is a condition that occurs when a patient incurs a second concussion before full recovery has occurred from an initial concussion. The second blow does not need to be forceful in order to cause SIS. SIS is considered rare but is a very serious condition and can result in death or severe brain damage as the brain rapidly swells and/or bleeds following the second blow. SIS occurs most often in young athletes under the age of approximately 25 and when it does occur has a high fatality rate among these athletes. Due to the real possibility of SIS a conservative rather than aggressive return to activity protocol should be implemented following a concussion.
Post Concussion Syndrome
Post concussion syndrome (PCS) is the presence of symptoms from a concussion, which last much longer than expected. Symptoms may last weeks, months, or occasionally even years. Symptoms are varied but can be physical, such as a headache or dizziness, or may be cognitive such as difficulty concentrating or performing mental tasks. Other symptoms such as light sensitivity, or emotional irritability may also occur.
The cause of PCS is unclear. One belief is that structural damage to the brain causes the ongoing symptoms. Others believe, however, that the symptoms develop due to a psychological or emotional reaction to the initial injury. In any case it is considered abnormal and a complication of a concussion.
Fortunately in most cases PCS symptoms resolve in approximately 3 months.
Depression
Depression has been reported as being a potential long-term consequence of concussion and when present, may be considered a symptom of PCS.
Further research is needed to accurately link concussions to a depressed state, however trends in research are focusing on the possibility that the greater the number of concussions sustained, the greater your risk for depression.
STAR Physical Therapy provides services for Physical Therapy in Fairport and Rochester.
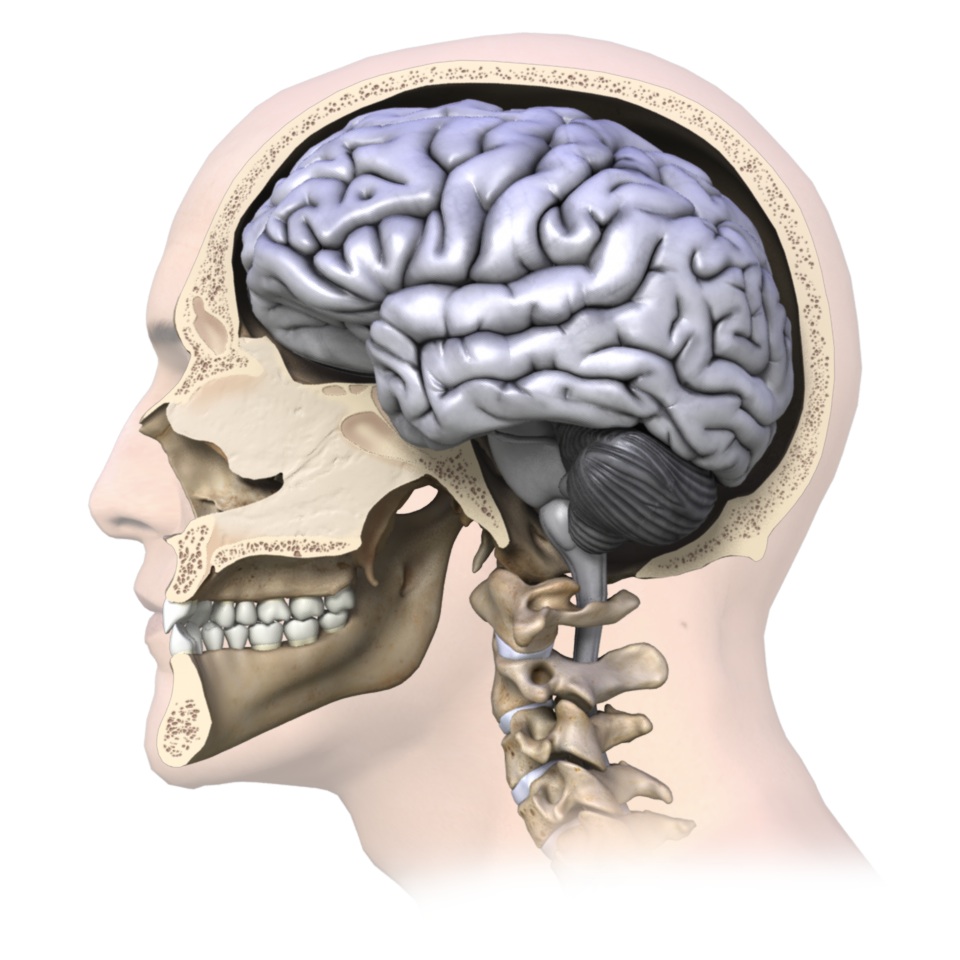
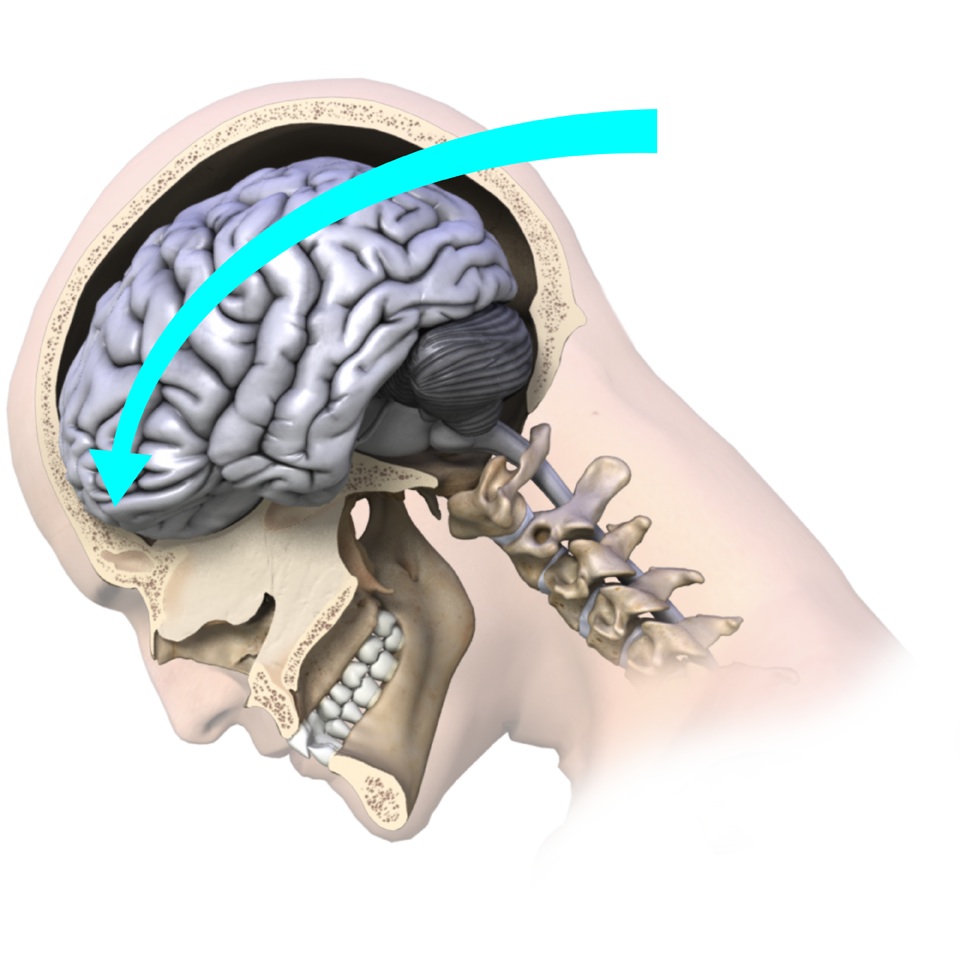 e that causes the brain to move rapidly within the skull and bang against the inside of the skull can cause a concussion. In layman’s terms, a concussion can be caused by anything that ‘rattles the brain.’
e that causes the brain to move rapidly within the skull and bang against the inside of the skull can cause a concussion. In layman’s terms, a concussion can be caused by anything that ‘rattles the brain.’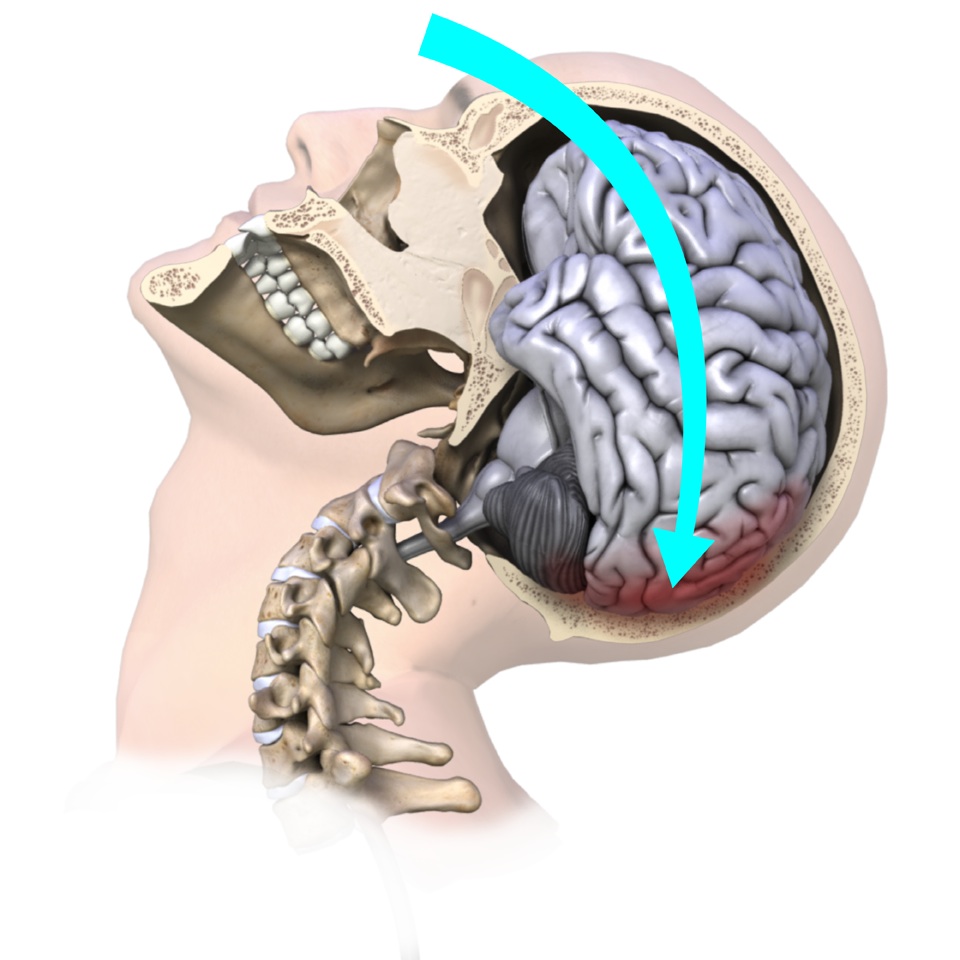 nts often similarly cause concussions due to the whiplash motion of your neck which subsequently forces your brain to rapidly hit the inside of your skull. Shaken baby syndrome is another example of this indirect mechanism of brain injury, as are explosions where your body is rapidly thrown back.
nts often similarly cause concussions due to the whiplash motion of your neck which subsequently forces your brain to rapidly hit the inside of your skull. Shaken baby syndrome is another example of this indirect mechanism of brain injury, as are explosions where your body is rapidly thrown back. fusion is another common sign. This sign can easily be overlooked by the examiner unless the patient is moderately to severely confused, so ruling out a concussion should not be based on the fact that the patient ‘did not appear confused.’
fusion is another common sign. This sign can easily be overlooked by the examiner unless the patient is moderately to severely confused, so ruling out a concussion should not be based on the fact that the patient ‘did not appear confused.’