Non-surgical Rehabilitation
Nonsurgical management of plantar fasciitis is successful in 90 per cent of all cases. When you begin therapy at STAR Physical Therapy, our Physical Therapist will design exercises to improve flexibility in the calf muscles, Achilles' tendon, and the plantar fascia.
We will apply treatments to the painful area to help control pain and swelling. Examples include ultrasound, ice packs, and soft-tissue massage. Our Physical Therapy sessions sometimes include iontophoresis, which uses a mild electrical current to push anti-inflammatory medicine, prescribed by your doctor, into the sore area.
We may have a customized arch support, or orthotic, designed to support the arch of your foot and to help cushion your heel. Supporting the arch with a well fitted orthotic may help reduce pressure on the plantar fascia. Alternatively, we may recommend placing a special type of insert into the shoe, called a heel cup. This device can also reduce the pressure on the sore area. Wearing a silicone heel pad adds cushion to a heel that has lost some of the fat pad through degeneration.
Your Physical Therapist will also provide ideas for therapies that you can perform at home, such as doing your stretches for the calf muscles and the plantar fascia. We may also have you fit with a night splint to wear while you sleep. The night splint keeps your foot from bending downward and places a mild stretch on the calf muscles and the plantar fascia. Some people seem to get better faster when using a night splint and report having less heel pain when placing the sore foot on the ground in the morning.
We find that many times it takes a combination of different approaches to get the best results for patients with plantar fasciitis. There isn’t a one-size-fits-all plan. Some patients do best with a combination of heel padding, medications, and stretching. If this doesn’t provide relief from symptoms within four to six weeks, then we may advise additional Physical Therapy and orthotics.
Finding the right combination for you may take some time. Don't be discouraged if it takes a few weeks to a few months to find the right fit for you. Most of the time, the condition is self-limiting. This means it doesn't last forever but does get better with a little time and attention. But in some cases, it can take up to a full year or more for the problem to be resolved.
Post-surgical Rehabilitation
Although recovery rates vary among patients, it generally takes several weeks before the tissues are well healed after surgery. The incision is protected with a bandage or dressing for about one week after surgery. You will probably use crutches briefly, and your Physical Therapist can help you learn to properly use your crutches to avoid placing weight of your foot while it heals.
The stitches are generally removed in 10 to 14 days. However, if your surgeon used sutures that dissolve, you won't need to have the stitches taken out. You should be released to full activity in about six weeks.
Surgical release of the plantar fascia decreases stiffness in the arch. However, it can also lead to collapse of the longitudinal (lengthwise) arch of the foot. Releasing the fascia alters the biomechanics of the foot and may decrease stability of the foot arch. The result may be increased stress on the other plantar ligaments and bones. Fractures and instability have been reported in up to 40 per cent of patients who have a plantar fasciotomy.
Throughout your post-surgical recovery, our Physical Therapist will note your progress and be watchful for the development of fractures and instability. When your recovery is well under way, regular visits to STAR Physical Therapy will end. Although we will continue to be a resource, you will eventually be in charge of doing some therapeutic exercises as part of an ongoing home program.
STAR Physical Therapy provides services for Physical Therapy in Fairport and Rochester.
 The
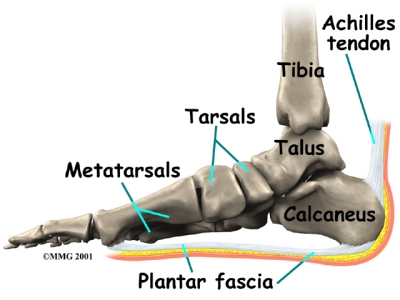
The 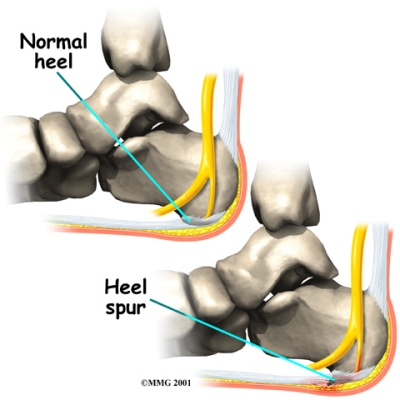 As you can imagine, when the foot is on the ground a tremendous amount of force (the full weight of the body) is concentrated on the plantar fascia. This force stretches the plantar fascia as the arch of the foot tries to flatten from the weight of your body. This is just how the string on a bow is stretched by the force of the bow trying to straighten. This leads to stress on the plantar fascia where it attaches to the heel bone. Small tears of the fascia can result. These tears are normally repaired by the body.
As you can imagine, when the foot is on the ground a tremendous amount of force (the full weight of the body) is concentrated on the plantar fascia. This force stretches the plantar fascia as the arch of the foot tries to flatten from the weight of your body. This is just how the string on a bow is stretched by the force of the bow trying to straighten. This leads to stress on the plantar fascia where it attaches to the heel bone. Small tears of the fascia can result. These tears are normally repaired by the body.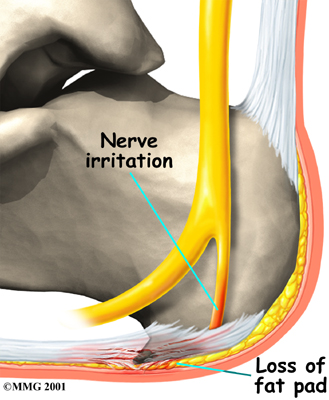
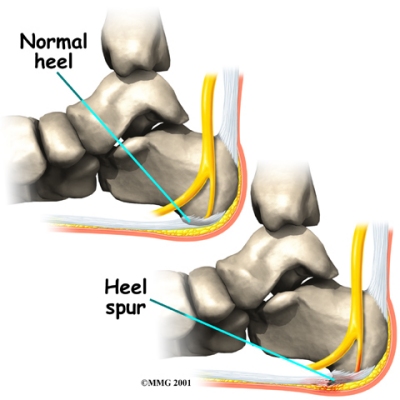 Your doctor may order an X-ray to rule out a stress fracture of the heel bone and to see if a
Your doctor may order an X-ray to rule out a stress fracture of the heel bone and to see if a